Magnesium

Detailed information about magnesium, the foods that provide magnesium, magnesium deficiency, and the best way to get extra magnesium.
Table of Contents
- Magnesium: What is it?
- What foods provide magnesium?
- What are the Dietary Reference Intakes for magnesium?
- When can magnesium deficiency occur?
- Who may need extra magnesium?
- What is the best way to get extra magnesium?
- What are some current issues and controversies about magnesium?
- What is the health risk of too much magnesium?
- Selecting a healthful diet
- References
Magnesium: What is it?
Magnesium is the fourth most abundant mineral in the body and is essential to good health. Approximately 50% of total body magnesium is found in bone. The other half is found predominantly inside cells of body tissues and organs. Only 1% of magnesium is found in blood, but the body works very hard to keep blood levels of magnesium constant [1].
Magnesium is needed for more than 300 biochemical reactions in the body. It helps maintain normal muscle and nerve function, keeps heart rhythm steady, supports a healthy immune system, and keeps bones strong. Magnesium also helps regulate blood sugar levels, promotes normal blood pressure, and is known to be involved in energy metabolism and protein synthesis [2-3]. There is an increased interest in the role of magnesium in preventing and managing disorders such as hypertension, cardiovascular disease, and diabetes. Dietary magnesium is absorbed in the small intestines. Magnesium is excreted through the kidneys [1-3,4].
What foods provide magnesium?
Green vegetables such as spinach are good sources of magnesium because the center of the chlorophyll molecule (which gives green vegetables their color) contains magnesium. Some legumes (beans and peas), nuts and seeds, and whole, unrefined grains are also good sources of magnesium [5]. Refined grains are generally low in magnesium [4-5]. When white flour is refined and processed, the magnesium-rich germ and bran are removed. Bread made from whole grain wheat flour provides more magnesium than bread made from white refined flour. Tap water can be a source of magnesium, but the amount varies according to the water supply. Water that naturally contains more minerals is described as "hard". "Hard" water contains more magnesium than "soft" water.
Eating a wide variety of legumes, nuts, whole grains, and vegetables will help you meet your daily dietary need for magnesium. Selected food sources of magnesium are listed in Table 1.
Table 1: Selected food sources of magnesium [5]
| FOOD | Milligrams (mg) | %DV* |
|---|---|---|
| Halibut, cooked, 3 ounces | 90 | 20 |
| Almonds, dry roasted, 1 ounce | 80 | 20 |
| Cashews, dry roasted, 1 ounce | 75 | 20 |
| Soybeans, mature, cooked, ½ cup | 75 | 20 |
| Spinach, frozen, cooked, ½ cup | 75 | 20 |
| Nuts, mixed, dry roasted, 1 ounce | 65 | 15 |
| Cereal, shredded wheat, 2 rectangular biscuits | 55 | 15 |
| Oatmeal, instant, fortified, prepared w/ water, 1 cup | 55 | 15 |
| Potato, baked w/ skin, 1 medium | 50 | 15 |
| Peanuts, dry roasted, 1 ounce | 50 | 15 |
| Peanut butter, smooth, 2 Tablespoons | 50 | 15 |
| Wheat Bran, crude, 2 Tablespoons | 45 | 10 |
| Blackeyed Peas, cooked, ½ cup | 45 | 10 |
| Yogurt, plain, skim milk, 8 fluid ounces | 45 | 10 |
| Bran Flakes, ¾ cup | 40 | 10 |
| Vegetarian Baked Beans, ½ cup | 40 | 10 |
| Rice, brown, long-grained, cooked, ½ cup | 40 | 10 |
| Lentils, mature seeds, cooked, ½ cup | 35 | 8 |
| Avocado, California, ½ cup pureed | 35 | 8 |
| Kidney Beans, canned, ½ cup | 35 | 8 |
| Pinto Beans, cooked, ½ cup | 35 | 8 |
| Wheat Germ, crude, 2 Tablespoons | 35 | 8 |
| Chocolate milk, 1 cup | 33 | 8 |
| Banana, raw, 1 medium | 30 | 8 |
| Milk Chocolate candy bar, 1.5 ounce bar | 28 | 8 |
| Milk, reduced fat (2%) or fat free, 1 cup | 27 | 8 |
| Bread, whole wheat, commercially prepared, 1 slice | 25 | 6 |
| Raisins, seedless, ¼ cup packed | 25 | 6 |
| Whole Milk, 1 cup | 24 | 6 |
| Chocolate Pudding, 4 ounce ready-to-eat portion | 24 | 6 |
*DV = Daily Value. DVs are reference numbers developed by the Food and Drug Administration (FDA) to help consumers determine if a food contains a lot or a little of a specific nutrient. The DV for magnesium is 400 milligrams (mg). Most food labels do not list a food's magnesium content. The percent DV (%DV) listed on the table above indicates the percentage of the DV provided in one serving. A food providing 5% of the DV or less per serving is a low source while a food that provides 10-19% of the DV is a good source. A food that provides 20% or more of the DV is high in that nutrient. It is important to remember that foods that provide lower percentages of the DV also contribute to a healthful diet. For foods not listed in this table, please refer to the U.S. Department of Agriculture's Nutrient Database Web site: http://www.nal.usda.gov/fnic/cgi-bin/nut_search.pl.
What are the Dietary Reference Intakes for magnesium?
Recommendations for magnesium are provided in the Dietary Reference Intakes (DRIs) developed by the Institute of Medicine of the National Academy of Sciences [4]. Dietary Reference Intakes is the general term for a set of reference values used for planning and assessing nutrient intake for healthy people. Three important types of reference values included in the DRIs are Recommended Dietary Allowances (RDA), Adequate Intakes (AI), and Tolerable Upper Intake Levels (UL). The RDA recommends the average daily intake that is sufficient to meet the nutrient requirements of nearly all (97-98%) healthy individuals in each age and gender group. An AI is set when there is insufficient scientific data available to establish a RDA for specific age/gender groups. AIs meet or exceed the amount needed to maintain a nutritional state of adequacy in nearly all members of a specific age and gender group. The UL, on the other hand, is the maximum daily intake unlikely to result in adverse health effects. Table 2 lists the RDAs for magnesium, in milligrams, for children and adults [4].
Table 2: Recommended Dietary Allowances for magnesium for children and adults [4]
| Age (years) | Male (mg/day) | Female (mg/day) | Pregnancy (mg/day) | Lactation (mg/day) |
|---|---|---|---|---|
| 1-3 | 80 | 80 | N/A | N/A |
| 4-8 | 130 | 130 | N/A | N/A |
| 9-13 | 240 | 240 | N/A | N/A |
| 14-18 | 410 | 360 | 400 | 360 |
| 19-30 | 400 | 310 | 350 | 310 |
| 31+ | 420 | 320 | 360 | 320 |
There is insufficient information on magnesium to establish a RDA for infants. For infants 0 to 12 months, the DRI is in the form of an Adequate Intake (AI), which is the mean intake of magnesium in healthy, breastfed infants. Table 3 lists the AIs for infants in milligrams (mg) [4].
Table 3: Recommended Adequate Intake for magnesium for infants [4]
| Age (months) | Males and Females (mg/day) |
|---|---|
| 0 to 6 | 30 |
| 7 to 12 | 75 |
Data from the 1999-2000 National Health and Nutrition Examination Survey suggest that substantial numbers of adults in the United States (US) fail to consume recommended amounts of magnesium. Among adult men and women, Caucasians consume significantly more magnesium than African-Americans. Magnesium intake is lower among older adults in every racial and ethnic group. African-American men and Caucasian men and women who take dietary supplements consume significantly more magnesium than those who do not [6].
When can magnesium deficiency occur?
Even though dietary surveys suggest that many Americans do not consume recommended amounts of magnesium, symptoms of magnesium deficiency are rarely seen in the US. However, there is concern about the prevalence of sub-optimal magnesium stores in the body. For many people, dietary intake may not be high enough to promote an optimal magnesium status, which may be protective against disorders such as cardiovascular disease and immune dysfunction [7-8].
The health status of the digestive system and the kidneys significantly influence magnesium status. Magnesium is absorbed in the intestines and then transported through the blood to cells and tissues. Approximately one-third to one-half of dietary magnesium is absorbed into the body [9-10]. Gastrointestinal disorders that impair absorption such as Crohn's disease can limit the body's ability to absorb magnesium. These disorders can deplete the body's stores of magnesium and in extreme cases may result in magnesium deficiency. Chronic or excessive vomiting and diarrhea may also result in magnesium depletion [1,10].
Healthy kidneys are able to limit urinary excretion of magnesium to compensate for low dietary intake. However, excessive loss of magnesium in urine can be a side effect of some medications and can also occur in cases of poorly-controlled diabetes and alcohol abuse [11-18].
Early signs of magnesium deficiency include loss of appetite, nausea, vomiting, fatigue, and weakness. As magnesium deficiency worsens, numbness, tingling, muscle contractions and cramps, seizures, personality changes, abnormal heart rhythms, and coronary spasms can occur [1,3-4]. Severe magnesium deficiency can result in low levels of calcium in the blood (hypocalcemia). Magnesium deficiency is also associated with low levels of potassium in the blood (hypokalemia) [1,19-20].
Many of these symptoms are general and can result from a variety of medical conditions other than magnesium deficiency. It is important to have a physician evaluate health complaints and problems so that appropriate care can be given.
Who may need extra magnesium?
Magnesium supplementation may be indicated when a specific health problem or condition causes an excessive loss of magnesium or limits magnesium absorption [2,7,9-11].
-
Some medicines may result in magnesium deficiency, including certain diuretics, antibiotics, and medications used to treat cancer (anti-neoplastic medication) [12,14,19]. Examples of these medications are:
-
Diuretics: Lasix, Bumex, Edecrin, and hydrochlorothiazide
-
Antibiotics: Gentamicin, and Amphotericin
-
Anti-neoplastic medication: Cisplatin
-
-
Individuals with poorly-controlled diabetes may benefit from magnesium supplements because of increased magnesium loss in urine associated with hyperglycemia [21].
-
Magnesium supplementation may be indicated for persons with alcoholism. Low blood levels of magnesium occur in 30% to 60% of alcoholics, and in nearly 90% of patients experiencing alcohol withdrawal [17-18]. Anyone who substitutes alcohol for food will usually have significantly lower magnesium intakes.
-
Individuals with chronic malabsorptive problems such as Crohn's disease, gluten sensitive enteropathy, regional enteritis, and intestinal surgery may lose magnesium through diarrhea and fat malabsorption [22]. Individuals with these conditions may need supplemental magnesium.
-
Individuals with chronically low blood levels of potassium and calcium may have an underlying problem with magnesium deficiency. Magnesium supplements may help correct the potassium and calcium deficiencies [19].
-
Older adults are at increased risk for magnesium deficiency. The 1999-2000 and 1998-94 National Health and Nutrition Examination Surveys suggest that older adults have lower dietary intakes of magnesium than younger adults [6,23]. In addition, magnesium absorption decreases and renal excretion of magnesium increases in older adults [4]. Seniors are also more likely to be taking drugs that interact with magnesium. This combination of factors places older adults at risk for magnesium deficiency [4]. It is very important for older adults to consume recommended amounts of dietary magnesium.
Doctors can evaluate magnesium status when above-mentioned medical problems occur, and determine the need for magnesium supplementation.
Table 4 describes some important interactions between certain drugs and magnesium. These interactions may result in higher or lower levels of magnesium, or may influence absorption of the medication.
Table 4: Common and important magnesium/drug interactions
| Drug | Potential Interaction |
|---|---|
| Loop and thiazide diuretics (e.g. lasix, bumex, edecrin, and hydrochlorthiazide Anti-neoplastic drugs (e.g. cisplatin) Antibiotics (e.g. gentamicin and amphotericin) | These drugs may increase the loss of magnesium in urine. Thus, taking these medications for long periods of time may contribute to magnesium depletion [9-10,12]. |
| Tetracycline antibiotics | Magnesium binds tetracycline in the gut and decreases the absorption of tetracycline [24]. |
| Magnesium-containing antacids and laxatives | Many antacids and laxatives contain magnesium. When frequently taken in large doses, these drugs can inadvertently lead to excessive magnesium consumption [25-26] and hypermagnesemia, which refers to elevated levels of magnesium in blood. |
What is the best way to get extra magnesium?
Eating a variety of whole grains, legumes, and vegetables (especially dark-green, leafy vegetables) every day will help provide recommended intakes of magnesium and maintain normal storage levels of this mineral. Increasing dietary intake of magnesium can often restore mildly depleted magnesium levels. However, increasing dietary intake of magnesium may not be enough to restore very low magnesium levels to normal.
When blood levels of magnesium are very low, intravenous (i.e. by IV) magnesium replacement is usually recommended. Magnesium tablets also may be prescribed, although some forms can cause diarrhea [27]. It is important to have the cause, severity, and consequences of low blood levels of magnesium evaluated by a physician, who can recommend the best way to restore magnesium levels to normal. Because people with kidney disease may not be able to excrete excess amounts of magnesium, they should not consume magnesium supplements unless prescribed by a physician.
Oral magnesium supplements combine magnesium with another substance such as a salt. Examples of magnesium supplements include magnesium oxide, magnesium sulfate, and magnesium carbonate. Elemental magnesium refers to the amount of magnesium in each compound. Figure 1 compares the amount of elemental magnesium in different types of magnesium supplements [28]. The amount of elemental magnesium in a compound and its bioavailability influence the effectiveness of the magnesium supplement. Bioavailability refers to the amount of magnesium in food, medications, and supplements that is absorbed in the intestines and ultimately available for biological activity in your cells and tissues. Enteric coating of a magnesium compound can decrease bioavailability [29]. In a study that compared four forms of magnesium preparations, results suggested lower bioavailability of magnesium oxide, with significantly higher and equal absorption and bioavailability of magnesium chloride and magnesium lactate [30]. This supports the belief that both the magnesium content of a dietary supplement and its bioavailability contribute to its ability to replete deficient levels of magnesium.
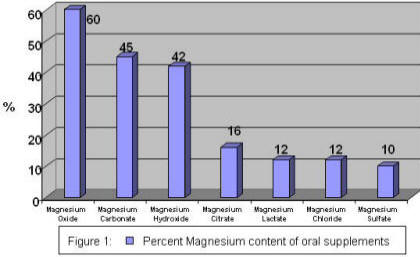
The information in Figure 1 is provided to demonstrate the variable amount of magnesium in magnesium supplements.
What are some current issues and controversies about magnesium?
Magnesium and blood pressure
"Epidemiologic evidence suggests that magnesium may play an important role in regulating blood pressure [4]." Diets that provide plenty of fruits and vegetables, which are good sources of potassium and magnesium, are consistently associated with lower blood pressure [31-33]. The DASH study (Dietary Approaches to Stop Hypertension), a human clinical trial, suggested that high blood pressure could be significantly lowered by a diet that emphasizes fruits, vegetables, and low fat dairy foods. Such a diet will be high in magnesium, potassium, and calcium, and low in sodium and fat [34-36].
An observational study examined the effect of various nutritional factors on incidence of high blood pressure in over 30,000 US male health professionals. After four years of follow-up, it was found that a lower risk of hypertension was associated with dietary patterns that provided more magnesium, potassium, and dietary fiber [37]. For 6 years, the Atherosclerosis Risk in Communities (ARIC) Study followed approximately 8,000 men and women who were initially free of hypertension. In this study, the risk of developing hypertension decreased as dietary magnesium intake increased in women, but not in men [38].
Foods high in magnesium are frequently high in potassium and dietary fiber. This makes it difficult to evaluate the independent effect of magnesium on blood pressure. However, newer scientific evidence from DASH clinical trials is strong enough that the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure states that diets that provide plenty of magnesium are positive lifestyle modifications for individuals with hypertension. This group recommends the DASH diet as a beneficial eating plan for people with hypertension and for those with "prehypertension" who desire to prevent high blood pressure http://www.nhlbi.nih.gov/health/public/heart/hbp/dash/ [39-41].
Magnesium and diabetes
Diabetes is a disease resulting in insufficient production and/or inefficient use of insulin. Insulin is a hormone made by the pancreas. Insulin helps convert sugar and starches in food into energy to sustain life. There are two types of diabetes: type 1 and type 2. Type 1 diabetes is most often diagnosed in children and adolescents, and results from the body's inability to make insulin. Type 2 diabetes, which is sometimes referred to as adult-onset diabetes, is the most common form of diabetes. It is usually seen in adults and is most often associated with an inability to use the insulin made by the pancreas. Obesity is a risk factor for developing type 2 diabetes. In recent years, rates of type 2 diabetes have increased along with the rising rates of obesity.
Magnesium plays an important role in carbohydrate metabolism. It may influence the release and activity of insulin, the hormone that helps control blood glucose (sugar) levels [13]. Low blood levels of magnesium (hypomagnesemia) are frequently seen in individuals with type 2 diabetes. Hypomagnesemia may worsen insulin resistance, a condition that often precedes diabetes, or may be a consequence of insulin resistance. Individuals with insulin resistance do not use insulin efficiently and require greater amounts of insulin to maintain blood sugar within normal levels. The kidneys possibly lose their ability to retain magnesium during periods of severe hyperglycemia (significantly elevated blood glucose). The increased loss of magnesium in urine may then result in lower blood levels of magnesium [4]. In older adults, correcting magnesium depletion may improve insulin response and action [42].
The Nurses' Health Study (NHS) and the Health Professionals' Follow-up Study (HFS) follow more than 170,000 health professionals through biennial questionnaires. Diet was first evaluated in 1980 in the NHS and in 1986 in the HFS, and dietary assessments have been completed every 2 to 4 years since. Information on the use of dietary supplements, including multivitamins, is also collected. As part of these studies, over 127,000 research subjects (85,060 women and 42,872 men) with no history of diabetes, cardiovascular disease, or cancer at baseline were followed to examine risk factors for developing type 2 diabetes. Women were followed for 18 years; men were followed for 12 years. Over time, the risk for developing type 2 diabetes was greater in men and women with a lower magnesium intake. This study supports the dietary recommendation to increase consumption of major food sources of magnesium, such as whole grains, nuts, and green leafy vegetables [43].
The Iowa Women's Health Study has followed a group of older women since 1986. Researchers from this study examined the association between women's risk of developing type 2 diabetes and intake of carbohydrates, dietary fiber, and dietary magnesium. Dietary intake was estimated by a food frequency questionnaire, and incidence of diabetes throughout 6 years of follow-up was determined by asking participants if they had been diagnosed by a doctor as having diabetes. Based on baseline dietary intake assessment only, researchers' findings suggested that a greater intake of whole grains, dietary fiber, and magnesium decreased the risk of developing diabetes in older women [44].
The Women's Health Study was originally designed to evaluate the benefits versus risks of low-dose aspirin and vitamin E supplementation in the primary prevention of cardiovascular disease and cancer in women 45 years of age and older. In an examination of almost 40,000 women participating in this study, researchers also examined the association between magnesium intake and incidence of type 2 diabetes over an average of 6 years. Among women who were overweight, the risk of developing type 2 diabetes was significantly greater among those with lower magnesium intake [45]. This study also supports the dietary recommendation to increase consumption of major food sources of magnesium, such as whole grains, nuts, and green leafy vegetables.
On the other hand, the Atherosclerosis Risk in Communities (ARIC) study did not find any association between dietary magnesium intake and the risk for type 2 diabetes. During 6 years of follow-up, ARIC researchers examined the risk for type 2 diabetes in over 12,000 middle-aged adults without diabetes at baseline examination. In this study, there was no statistical association between dietary magnesium intake and incidence of type 2 diabetes in either black or white research subjects [46]. It can be confusing to read about studies that examine the same issue but have different results. Before reaching a conclusion on a health issue, scientists conduct and evaluate many studies. Over time, they determine when results are consistent enough to suggest a conclusion. They want to be sure they are providing correct recommendations to the public.
Several clinical studies have examined the potential benefit of supplemental magnesium on metabolic control of type 2 diabetes. In one such study, 63 subjects with below normal serum magnesium levels received either 2.5 grams of oral magnesium chloride daily "in liquid form" (providing 300 mg elemental magnesium per day) or a placebo. At the end of the 16-week study period, those who received the magnesium supplement had higher blood levels of magnesium and improved metabolic control of diabetes, as suggested by lower Hemoglobin A1C levels, than those who received a placebo [47]. Hemoglobin A1C is a test that measures overall control of blood glucose over the previous 2 to 3 months, and is considered by many doctors to be the single most important blood test for diabetics.
In another study, 128 patients with poorly controlled type 2 diabetes were randomized to receive a placebo or a supplement with either 500 mg or 1000 mg of magnesium oxide (MgO) for 30 days. All patients were also treated with diet or diet plus oral medication to control blood glucose levels. Magnesium levels increased in the group receiving 1000 mg magnesium oxide per day (equal to 600 mg elemental magnesium per day) but did not significantly change in the placebo group or the group receiving 500 mg of magnesium oxide per day (equal to 300 mg elemental magnesium per day). However, neither level of magnesium supplementation significantly improved blood glucose control [48].
These studies provide intriguing results but also suggest that additional research is needed to better explain the association between blood magnesium levels, dietary magnesium intake, and type 2 diabetes. In 1999, the American Diabetes Association (ADA) issued nutrition recommendations for diabetics stating that "...routine evaluation of blood magnesium level is recommended only in patients at high risk for magnesium deficiency. Levels of magnesium should be repleted (replaced) only if hypomagnesemia can be demonstrated" [21].
Magnesium and cardiovascular disease
Magnesium metabolism is very important to insulin sensitivity and blood pressure regulation, and magnesium deficiency is common in individuals with diabetes. The observed associations between magnesium metabolism, diabetes, and high blood pressure increase the likelihood that magnesium metabolism may influence cardiovascular disease [49].
Some observational surveys have associated higher blood levels of magnesium with lower risk of coronary heart disease [50-51]. In addition, some dietary surveys have suggested that a higher magnesium intake may reduce the risk of having a stroke [52]. There is also evidence that low body stores of magnesium increase the risk of abnormal heart rhythms, which may increase the risk of complications after a heart attack [4]. These studies suggest that consuming recommended amounts of magnesium may be beneficial to the cardiovascular system. They have also prompted interest in clinical trials to determine the effect of magnesium supplements on cardiovascular disease.
Several small studies suggest that magnesium supplementation may improve clinical outcomes in individuals with coronary disease. In one of these studies, the effect of magnesium supplementation on exercise tolerance, exercise-induced chest pain, and quality of life was examined in 187 patients. Patients received either a placebo or a supplement providing 365 milligrams of magnesium citrate twice daily for 6 months. At the end of the study period researchers found that magnesium therapy significantly increased magnesium levels. Patients receiving magnesium had a 14 percent improvement in exercise duration as compared to no change in the placebo group. Those receiving magnesium were also less likely to experience exercise-induced chest pain [53].
In another study, 50 men and women with stable coronary disease were randomized to receive either a placebo or a magnesium supplement that provided 342 mg magnesium oxide twice daily. After 6 months, those who received the oral magnesium supplement were found to have improved exercise tolerance [54].
In a third study, researchers examined whether magnesium supplementation would add to the anti-thrombotic (anti-clotting) effects of aspirin in 42 coronary patients [55]. For three months, each patient received either a placebo or a supplement with 400 mg of magnesium oxide two to three times daily. After a four-week break without any treatment, treatment groups were reversed so that each person in the study then received the alternate treatment for three months. Researchers found that supplemental magnesium did provide an additional anti-thrombotic effect.
These studies are encouraging, but involved small numbers. Additional studies are needed to better understand the complex relationships between magnesium intake, indicators of magnesium status, and heart disease. Doctors can evaluate magnesium status when above-mentioned medical problems occur, and determine the need for magnesium supplementation.
Magnesium and osteoporosis
Bone health is supported by many factors, most notably calcium and vitamin D. However, some evidence suggests that magnesium deficiency may be an additional risk factor for postmenopausal osteoporosis [4]. This may be due to the fact that magnesium deficiency alters calcium metabolism and the hormones that regulate calcium (20). Several human studies have suggested that magnesium supplementation may improve bone mineral density [4]. In a study of older adults, a greater magnesium intake maintained bone mineral density to a greater degree than a lower magnesium intake [56]. Diets that provide recommended levels of magnesium are beneficial for bone health, but further investigation on the role of magnesium in bone metabolism and osteoporosis is needed.
What is the health risk of too much magnesium?
Dietary magnesium does not pose a health risk, however pharmacologic doses of magnesium in supplements can promote adverse effects such as diarrhea and abdominal cramping. Risk of magnesium toxicity increases with kidney failure, when the kidney loses the ability to remove excess magnesium. Very large doses of magnesium-containing laxatives and antacids also have been associated with magnesium toxicity [25]. For example, a case of hypermagnesemia after unsupervised intake of aluminum magnesia oral suspension occurred after a 16 year old girl decided to take the antacid every two hours rather than four times per day, as prescribed. Three days later, she became unresponsive and demonstrated loss of deep tendon reflex [57]. Doctors were unable to determine her exact magnesium intake, but the young lady presented with blood levels of magnesium five times higher than normal [25]. Therefore, it is important for medical professionals to be aware of the use of any magnesium-containing laxatives or antacids. Signs of excess magnesium can be similar to magnesium deficiency and include changes in mental status, nausea, diarrhea, appetite loss, muscle weakness, difficulty breathing, extremely low blood pressure, and irregular heartbeat [5,57-60].
Table 5 lists the ULs for supplemental magnesium for healthy infants, children, and adults in milligrams (mg) [4]. Physicians may prescribe magnesium in higher doses for specific medical problems. There is no UL for dietary intake of magnesium; only for magnesium supplements.
Table 5: Tolerable Upper Intake Levels for supplemental magnesium for children and adults [4]
| Age (years) | Male (mg/day) | Female (mg/day) | Pregnancy (mg/day) | Lactation (mg/day) |
|---|---|---|---|---|
| Infants | Undetermined | Undetermined | N/A | N/A |
| 1-3 | 65 | 65 | N/A | N/A |
| 4 - 8 | 110 | 110 | N/A | N/A |
| 9 - 18 | 350 | 350 | 350 | 350 |
| 19+ | 350 | 350 | 350 | 350 |
Selecting a healthful diet
The 2000 Dietary Guidelines for Americans states, "Different foods contain different nutrients and other healthful substances. No single food can supply all the nutrients in the amounts you need" [61]. If you want more information about building a healthful diet, refer to the Dietary Guidelines for Americans [61] (http://www.usda.gov/cnpp/DietGd.pdf) and the US Department of Agriculture's Food Guide Pyramid [62] (http://www.nal.usda.gov/fnic/Fpyr/pyramid.html).
back to: Alternative Medicine Home ~ Alternative Medicine Treatments
Source: Office of Dietary Supplements - National Institutes of Health
back to: Alternative Medicine Home ~ Alternative Medicine Treatments
References
- Rude RK. Magnesium deficiency: A cause of heterogeneous disease in humans. J Bone Miner Res 1998;13:749-58. [PubMed abstract]
- Wester PO. Magnesium. Am J Clin Nutr 1987;45:1305-12. [PubMed abstract]
- Saris NE, Mervaala E, Karppanen H, Khawaja JA, Lewenstam A. Magnesium: an update on physiological, clinical, and analytical aspects. Clinica Chimica Acta 2000;294:1-26.
- Institute of Medicine. Food and Nutrition Board. Dietary Reference Intakes: Calcium, Phosphorus, Magnesium, Vitamin D and Fluoride. National Academy Press. Washington, DC, 1999.
- U.S. Department of Agriculture, Agricultural Research Service. 2003. USDA National Nutrient Database for Standard Reference, Release 16. Nutrient Data Laboratory Home Page, http://www.nal.usda.gov/fnic/foodcomp.
- Ford ES and Mokdad AH. Dietary magnesium intake in a national sample of U.S. adults. J Nutr. 2003;133:2879-82.
- Vormann J. Magnesium: nutrition and metabolism. Molecular Aspects of Medicine 2003:24:27-37.
- Feillet-Coudray C, Coudray C, Tressol JC, Pepin D, Mazur A, Abrams SA. Exchangeable magnesium pool masses in healthy women: effects of magnesium supplementation. Am J Clin Nutr 2002;75:72-8.
- Ladefoged K, Hessov I, Jarnum S. Nutrition in short-bowel syndrome. Scand J Gastroenterol Suppl 1996;216:122-31. [PubMed abstract]
- Rude KR. Magnesium metabolism and deficiency. Endocrinol Metab Clin North Am 1993;22:377-95.
- Kelepouris E and Agus ZS. Hypomagnesemia: Renal magnesium handling. Semin Nephrol 1998;18:58-73. [PubMed abstract]
- Ramsay LE, Yeo WW, Jackson PR. Metabolic effects of diuretics. Cardiology 1994;84 Suppl 2:48-56. [PubMed abstract]
- Kobrin SM and Goldfarb S. Magnesium Deficiency. Semin Nephrol 1990;10:525-35. [PubMed abstract]
- Lajer H and Daugaard G. Cisplatin and hypomagnesemia. Ca Treat Rev 1999;25:47-58. [PubMed abstract]
- Tosiello L. Hypomagnesemia and diabetes mellitus. A review of clinical implications. Arch Intern Med 1996;156:1143-8. [PubMed abstract]
- Paolisso G, Scheen A, D'Onofrio F, Lefebvre P. Magnesium and glucose homeostasis. Diabetologia 1990;33:511-4. [PubMed abstract]
- Elisaf M, Bairaktari E, Kalaitzidis R, Siamopoulos K. Hypomagnesemia in alcoholic patients. Alcohol Clin Exp Res 1998;22:244-6. [PubMed abstract]
- Abbott L, Nadler J, Rude RK. Magnesium deficiency in alcoholism: Possible contribution to osteoporosis and cardiovascular disease in alcoholics. Alcohol Clin Exp Res 1994;18:1076-82. [PubMed abstract]
- Shils ME. Magnesium. In Modern Nutrition in Health and Disease, 9th Edition. (edited by Shils, ME, Olson, JA, Shike, M, and Ross, AC.) New York: Lippincott Williams and Wilkins, 1999, p. 169-92.
- Elisaf M, Milionis H, Siamopoulos K. Hypomagnesemic hypokalemia and hypocalcemia: Clinical and laboratory characteristics. Mineral Electrolyte Metab 1997;23:105-12. [PubMed abstract]
- American Diabetes Association. Nutrition recommendations and principles for people with diabetes mellitus. Diabetes Care 1999;22:542-5. [PubMed abstract]
- Rude RK and Olerich M. Magnesium deficiency: Possible role in osteoporosis associated with gluten-sensitive enteropathy. Osteoporos Int 1996;6:453-61. [PubMed abstract]
- Bialostosky K, Wright JD, Kennedy-Stephenson J, McDowell M, Johnson CL. Dietary intake of macronutrients, micronutrients and other dietary constituents: United States 1988-94. Vital Heath Stat. 11(245) ed: National Center for Health Statistics, 2002:168.
- Takahashi M, Degenkolb J, Hillen W. Determination of the equilibrium association constant between Tet repressor and tetracycline at limiting Mg2+ concentrations: a generally applicable method for effector-dependent high-affinity complexes. Anal Biochem 1991;199:197-202.
- Xing JH and Soffer EE. Adverse effects of laxatives. Dis Colon Rectum 2001;44:1201-9.
- Qureshi T and Melonakos TK. Acute hypermagnesemia after laxative use. Ann Emerg Med 1996;28:552-5. [PubMed abstract]
- DePalma J. Magnesium Replacement Therapy. Am Fam Phys 1990;42:173-6.
- Klasco RK (Ed): USP DI® Drug Information for the Healthcare Professional. Thomson MICROMEDEX, Greenwood Village, Colorado 2003.
- Fine KD, Santa Ana CA, Porter JL, Fordtran JS. Intestinal absorption of magnesium from food and supplements. J Clin Invest 1991;88:296-402.
- Firoz M and Graber M. Bioavailaility of US commercial magnesium preparation. Magnes Res 2001;14:257-62.
- Appel LJ. Nonpharmacologic therapies that reduce blood pressure: A fresh perspective. Clin Cardiol 1999;22:1111-5. [PubMed abstract]
- Simopoulos AP. The nutritional aspects of hypertension. Compr Ther 1999;25:95-100. [PubMed abstract]
- Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Sacks FM, Bray GA, Vogt TM, Cutler JA, Windhauser MM, Lin PH, Karanja N. A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med 1997;336:1117-24. [PubMed abstract]
- Sacks FM, Obarzanek E, Windhauser MM, Svetkey LP, Vommer WM, McCullough M, Karanja N, Lin PH, Steele P, Praschen MA, Evans M, Appel LJ, Bray GA, Vogt T, Moore MD for the DASH investigators. Rationale and design of the Dietary Approaches to Stop Hypertension trial (DASH). A multicenter controlled-feeding study of dietary patterns to lower blood pressure. Ann Epidemiol 1995;5:108-18. [PubMed abstract]
- Sacks FM, Appel LJ, Moore TJ, Obarzanek E, Vollmer WM, Svetkey LP, Bray GA, Vogt TM, Cutler JA, Windhauser MM, Lin PH, Karanja N. A dietary approach to prevent hypertension: A review of the Dietary Approaches to Stop Hypertension (DASH) Study. Clin Cardiol 1999;22:6-10. [PubMed abstract]
- Svetkey LP, Simons-Morton D, Vollmer WM, Appel LJ, Conlin PR, Ryan DH, Ard J, Kennedy BM. Effects of dietary patterns on blood pressure: Subgroup analysis of the Dietary Approaches to Stop Hypertension (DASH) randomized clinical trial. Arch Intern Med 1999;159:285-93. [PubMed abstract]
- Ascherio A, Rimm EB, Giovannucci EL, Colditz GA, Rosner B, Willett WC, Sacks FM, Stampfer MJ. A prospective study of nutritional factors and hypertension among US men. Circulation 1992;86:1475-84. [PubMed abstract]
- Peacock JM, Folsom AR, Arnett DK, Eckfeldt JH, Szklo M. Relationship of serum and dietary magnesium to incident hypertension: the Atherosclerosis Risk in Communities (ARIC) Study. Annals of Epidemiology 1999;9:159-65.
- National Heart, Lung, and Blood Institute. Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch Intern Med 1997;157:2413-46. [PubMed abstract]
- Schwartz GL and Sheps SG. A review of the sixth report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Curr Opin Cardiol 1999;14:161-8. [PubMed abstract]
- Kaplan NM. Treatment of hypertension: Insights from the JNC-VI report. Am Fam Physician 1998;58:1323-30. [PubMed abstract]
- Paolisso G, Sgambato S, Gambardella A, Pizza G, Tesauro P, Varricchio H, D'Onofrio F. Daily magnesium supplements improve glucose handling in elderly subjects. Am J Clin Nutr 1992;55:1161-7. [PubMed abstract]
- Lopez-Ridaura R, Willett WC, Rimm EB, Liu S, Stampfer MJ, Manson JE, Hu FB. Magnesium intake and risk of type 2 diabetes in men and women. Diabetes Care 2004;27:134-40.
- Meyer KA, Kishi LH, Jacobs DR Jr., Slavin J, Sellers TA, Folsom AR. Carbohydrates, dietary fiber, and incident type 2 diabetes in older women. Am J Clin Nutr 1999;71:921-30.
- Song V, Manson JE, Buring JE, Liu S. Dietary magnesium intake in relation to plasma insulin levels and risk of type 2 diabetes in women. Diabetes Care 2003;27:59-65.
- Kao WHL, Folsom AR, Nieto FJ, MO JP, Watson RL, Brancati FL. Serum and dietary magnesium and the risk for type 2 diabetes: The Atherosclerosis Risk in Communities Study. Arch Intern Med 1999;159:2151-59.
- Rodriguez-Moran M and Guerrero-Romero F. Oral magnesium supplementation improves insulin sensitivity and metabolic control in type 2 diabetic subjects. Diabetes Care 2003;26:1147-52.
- De Lourdes Lima, M, Cruz T, Pousada JC, Rodrigues LE, Barbosa K, Canguco V. The effect of magnesium supplementation in increasing doses on the control of type 2 diabetes. Diabetes Care 1998;21:682-86.
- Altura BM and Altura BT. Magnesium and cardiovascular biology: An important link between cardiovascular risk factors and atherogenesis. Cell Mol Biol Res 1995;41:347-59. [PubMed abstract]
- Ford ES. Serum magnesium and ischaemic heart disease: Findings from a national sample of US adults. Intl J of Epidem 1999;28:645-51. [PubMed abstract]
- Liao F, Folsom A, Brancati F. Is low magnesium concentration a risk factor for coronary heart disease? The Atherosclerosis Risk in Communities (ARIC) Study. Am Heart J 1998;136:480-90. [PubMed abstract]
- Ascherio A, Rimm EB, Hernan MA, Giovannucci EL, Kawachi I, Stampfer MJ, Willett WC. Intake of potassium, magnesium, calcium, and fiber and risk of stroke among US men. Circulation 1998;98:1198-204. [PubMed abstract]
- Shechter M, Bairey Merz CN, Stuehlinger HG, Slany J, Pachinger O, Rabinowitz B. Effects of oral magnesium therapy on exercise tolerance, exercise-induced chest pain, and quality of life in patients with coronary artery disease. Am J Cardiol 2003;91:517-21.
- Shechter M, Sharir M, Labrador MJ, Forrester J, Silver B, Bairey Merz CN. Oral magnesium therapy improves endothelial function in patients with coronary artery disease. Circulation 2000;102:2353-58.
- Shechter M, Merz CN, Paul-Labrador M, Meisel SR, Rude RK, Molloy MD, Dwyer JH, Shah PK, Kaul S. Oral magnesium supplementation inhibits platelet-dependent thrombosis in patients with coronary artery disease. American Journal of Cardiology 1999;84:152-6.
- Tucker KL, Hannan MT, Chen H, Cupples LA, Wilson PW, Kiel DP. Potassium, magnesium, and fruit and vegetable intakes are associated with greater bone mineral density in elderly men and women. Am J Clin Nutr 1999;69(4):727-36.
- Jaing T-H, Hung I-H, Chung H-T, Lai C-H, Liu W-M, Chang K-W. Acute hypermagnesemia: a rare complication of antacid administration after bone marrow transplantation. Clinica Chimica Acta 2002;326:201-3.
- Whang R. Clinical disorders of magnesium metabolism. Compr Ther 1997;23:168-73. [PubMed abstract]
- Ho J, Moyer TP, Phillips S. Chronic diarrhea: The role of magnesium. Mayo Clin Proc 1995;70:1091-2. [PubMed abstract]
- Nordt S, Williams SR, Turchen S, Manoguerra A, Smith D, Clark R. Hypermagnesemia following an acute ingestion of Epsom salt in a patient with normal renal function. J Toxicol Clin Toxicol 1996;34:735-9. [PubMed abstract]
- Dietary Guidelines Advisory Committee, Agricultural Research Service, United States Department of Agriculture (USDA). HG Bulletin No. 232, 2000. http://www.usda.gov/cnpp/DietGd.pdf.
- Center for Nutrition Policy and Promotion, United Stated Department of Agriculture. Food Guide Pyramid, 1992 (slightly revised 1996). http://www.nal.usda.gov/fnic/Fpyr/pyramid.html.
About ODS an the NIH Clinical Center
Disclaimer
Reasonable care has been taken in preparing this document and the information provided herein is believed to be accurate. However, this information is not intended to constitute an "authoritative statement" under Food and Drug Administration rules and regulations.
The mission of the Office of Dietary Supplements (ODS) is to strengthen knowledge and understanding of dietary supplements by evaluating scientific information, stimulating and supporting research, disseminating research results, and educating the public to foster an enhanced quality of life and health for the U.S. population.
The NIH Clinical Center is the clinical research hospital for NIH. Through clinical research, physicians and scientist translate laboratory discoveries into better treatments, therapies and interventions to improve the nation's health.
General Safety Advisory
Health professionals and consumers need credible information to make thoughtful decisions about eating a healthful diet and using vitamin and mineral supplements. To help guide those decisions, registered dietitians at the NIH Clinical Center developed a series of Fact Sheets in conjunction with ODS. These Fact Sheets provide responsible information about the role of vitamins and minerals in health and disease. Each Fact Sheet in this series received extensive review by recognized experts from the academic and research communities.
The information is not intended to be a substitute for professional medical advice. It is important to seek the advice of a physician about any medical condition or symptom. It is also important to seek the advice of a physician, registered dietitian, pharmacist, or other qualified health professional about the appropriateness of taking dietary supplements and their potential interactions with medications.
back to: Alternative Medicine Home ~ Alternative Medicine Treatments
APA Reference
Staff, H.
(2008, November 18). Magnesium, HealthyPlace. Retrieved
on 2026, August 6 from https://www.healthyplace.com/alternative-mental-health/treatments/magnesium

